Lithium (di)silicate: Strength & Aesthetics
By Dr José Ignacio Zorzin, Germany
The combination of modern nanohybrid composites and adhesive systems makes it possible to directly restore almost any tooth, preserving it with minimal invasiveness. However, if the tooth structure defect is so significant that it is not possible to establish sufficient proximal contact directly or if the functional design of the occlusal surface and cusps can only be achieved sub-optimally, a direct adhesive restoration is no longer the best treatment option. For these cases, indirect, adhesive tooth-coloured restorations such as ceramic inlays, onlays, and crowns are an ideal solution.
Lithium (di)silicate ceramics
Most dental ceramics have two phases: a glass and a crystalline phase. If the crystalline phase is produced by a thermal process (nucleation and crystallisation), these
materials are called glass ceramics. The glass phase is crucial for the aesthetics of the material: it gives the material its colour and its translucency. Unfortunately, it has relatively low strength and resistance to fractures due to its amorphous structure. The strength of glass ceramics results from the crystalline phase, which gives the material the necessary toughness to withstand masticatory forces. The higher the proportion of the crystalline phase, the better the mechanical properties of the ceramic. (Serbena et al., 2015) However, the crystallites scatter the incoming light and make the material opaque. The tooth-like aesthetics and mechanical properties of a glass ceramics result from the interaction of the two phases. Dental glass ceramics, such as leucite (Initial LRF, GC Corp, IPS Empress Press or CAD, Ivoclar Vivadent) or feldspar ceramics (Vita blocs Mark II, Vita Zahnfabrik) have a crystallite content of approximately 40% by volume. (Guazzato et al., 2004) They exhibit excellent aesthetics with high translucency and show a fracture toughness of approximately 1 MPa•m1/2. (Belli et al., 2018) Reinforced glass ceramics, such as lithium (di)silicate ceramics, have a considerably increased crystallite content of approximately 70% by volume and therefore show significantly higher fracture toughness compared to feldspar and leucite glass ceramics. (Belli et al., 2018) Due to their toughness and aesthetics, lithium (di)silicate ceramics are the material of choice for full crowns in the premolar, molar, and anterior, as well as for inlays, onlays, and overlays.
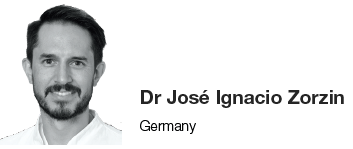
The higher mechanical properties of lithium (di)silicate ceramics rely on not only the higher crystallite content but also the microstructure of the crystallites. This glass ceramic contains crystallites of lithium silicate (Li2SiO3) and lithium disilicate (Li2SiO5), which have an elongated form (Fig. 1). These elongated crystallites form an interlocking bulk microstructure, which hinders the growth of potential cracks by deflection around the crystallites. (Belli et al., 2017) The improved mechanical properties of lithium disilicate compared to those of leucite ceramics are also reflected in everyday clinical practise: partial crowns made of milled lithium disilicate ceramics show a significantly higher survival rate than partial crowns made of milled leucite ceramics. (Belli et al., 2016)
Depending on the manufacturer, these reinforced modern glass ceramics are available as pressed ceramic (e.g., Initial LiSi Press, GC, Fig. 2a) or as CAD/ CAM blocks (Initial
LiSi Block, GC, Fig. 2b). Because some lithium (di)silicate ceramics are too hard, they are milled in a pre-crystallised form (e.g., IPS e.max CAD, Ivoclar Vivadent). After milling, a crystallisation firing is performed to ensure that the restoration retains its final aesthetics and strength ("two- step-chairside", CAD/CAM ceramics). Other variants (e.g., Initial LiSi Block, GC) do not require separate crystallisation firing ("one-step-chairside" CAD/CAM ceramics) and they can be postprocessed immediately after milling, by painting (e.g. Initial Lustre pastes ONE, GC), micro-layering (Lustre Pastes ONE and SQIN ceramics, GC) or simply by polishing to high gloss. The latter procedure probably also has clinical advantages: In vitro studies show that pure polish leads to less abrasion of the antagonists in the area of the contact points. (Lawson et al., 2014).
Cavity design
To reach a maximum of fracture resistance and aesthetics, tooth coloured partial crowns should be adhesively attached to the tooth. If a conventional adhesive luting of the restoration is intended (acid-etching of the tooth and dentine bonding), it is recommended to check if rubber dam can be placed (e.g., for inlays and onlays). In cases where subgingival preparation margins cannot be kept dry with a rubber dam, a "proximal box elevation" can be performed. In this case, a direct adhesive filling is placed using a matrix technique, which moves the preparation margin further coronally, so that rubber dam placement is possible. (Frankenberger et al., 2013) Generally, the preparation of tooth-coloured partial crowns is based on the preparation rules for ceramic inlays and partial crowns. (Frankenberger, 2007) The most important rule is that all transitions in the cavity are rounded to minimise stress peaks. The preparation should be designed so that the restoration always has a minimum layer thickness of 1.0-1.5 (in accordance with the manufacturer's recommendations for partial crowns) especially in the area of the central fissure, one should be aware to leave sufficient space. The residual tooth structure in the cusp area should not be less than 1.5 mm thick either. If this is not reached or if the preparation margin reaches the tip of the cusp, the cusp must be shortened. An angle of 90° should be created at the transition from the restoration to the hard tooth substance. The opening angle of the proximal cavities should also be 90°. The opening angle of the cavity wall to the occlusal should be 6 to 10°. Adhesive luting of lithium (di) silicate ceramics.
Lithium (di)silicate glass ceramics can be relatively easily adhesively luted to the tooth. Regardless of the method for adhesive luting, the correct pre-treatment of the restoration is crucial. Lithium (di)silicate ceramics are etched with 5% hydrofluoric acid according to the respective manufacturer's instructions and then thoroughly rinsed with water spray.
Hydrofluoric acid dissolves the glass phase from the surface and creates a rough micro-retentive surface. This surface is treated with a silane containing adhesion promoter. By evaporation of the solvents in the silane primer, the silanol group of silane condenses and chemically bonds with the etched glass-ceramic surface. The methacrylate residue of the silane coupling agent points toward the adhesive joint, where it can polymerise with the luting composite. This process is called salinisation.
Pre-treatment of the tooth and luting materials
Maximum adhesion to the tooth is required for inlays, onlays, and veneers so that the lithium (di)silicate ceramic can achieve its maximum strength and aesthetics. For this purpose, the tooth should be pre-treated by enamel etching technique and dentine bonding. For these procedures, an absolute dry field technique by means of a rubber dam is indispensable. (Falacho et al., 2023) For inlays, onlays and veneers, adhesive / multistep cements (e.g., G-CEM Link Force, G-CEM Veneer, GC; Multilink Automix, Variolink
Aesthetic, Ivoclar; RelyX Ultimate, 3M) and universal cements with adhesive/primer (G-CEM ONE with AEP or G-Premio Bond, GC Corp; RelyX Universal and Scotchbond Universal Plus, 3M) can be used. (Maravic et al., 2023)
When luting full crowns of lithium (di) silicate ceramics, where no enamel is left and sufficient retention is given, no pre-treatment of the tooth is required and self-adhesive/one-step cements (RelyX Unicem Automix 2, 3M) or universal cements in self-adhesive mode (G-CEM ONE, GC; RelyX Universal, 3M) can be the materials of choice. (Maravic et al., 2023)
Polish
The fitting of the restoration to the cavity or adjustment of the occlusion after placement is often unavoidable. Studies show that this can damage the surfaces of the ceramics to such an extent that their strength is permanently reduced,
and the probability of fractures increases. For this reason, the restoration should be perfectly polished after grinding, from the red band to the yellow band, and finally to the white band finishing bur. Simple polishing on a roughly ground restoration is not sufficient. Although it appears glossy to the eye, it leaves deep defects on the surface. (Lohbauer, 2018)
The Clinical Case
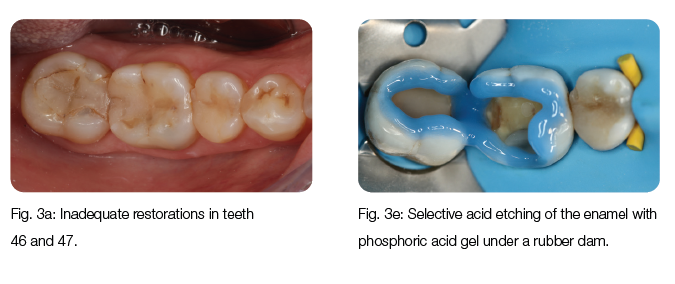
Inadequate restorations of teeth 46 and 47 had to be replaced (Fig. 3a). After the removal of the deficient restorations and caries, the decision was made to restore the teeth with two lithium disilicate press ceramic inlays (Initial LiSi Press, GC, Fig. 3b), due to the extent of the cavities. After try-in, the inlays were etched (Fig. 3c) with 5% hydrofluoric acid for
20 seconds and silanised (G-Multi PRIMER, GC Corp., Fig. 3d). After isolation of the teeth with rubber dam, the enamel surfaces of the cavity were selectively etched with 35% phosphoric acid gel (Fig. 3e). The cavity was pre-treated with an adhesive primer (G-CEM ONE AEP, GC, Fig. 3f) for subsequent luting with universal cement (G-CEM ONE, GC). After luting using the tack-cure technique, excesses of universal cement were removed and the teeth and restorations polished. After removal of the rubber dam, the restoration fitted nicely in the tooth (Fig. 3g).
Conclusions
Lithium (di)silicate glass ceramics are the ideal material for indirect tooth coloured restorations like inlays, onlays, and crowns because of the gentle aesthetics paired with toughness. Knowledge of the correct cavity design and adhesive procedures is essential for the best long-term performance in clinics.
Author Bio:
Priv.-Doz. Dr José Ignacio Zorzin is a senior dentist, researcher, and lecturer at the Department for Operative Dentistry at the University Hospital of Erlangen. His research topics include adhesive luting of indirect restorative materials, ceramics, and composites. His main clinical topics are minimally invasive aesthetic restorative procedures, endodontics, and dental photography. Dr Zorzin passed his state examination with distinction in 2009, received his doctorate in 2011 on the topic of dental adhesives, and received his Venia legendi (habilitation) in 2019 on the topic of dental materials in modern dentistry. He regularly publishes in scientific journals and is a sought-after speaker at conferences and continuing education courses.
REFERENCES:
BELLI, R., PETSCHELT, A., HOFNER, B., HAJTO, J., SCHERRER, S. S. & LOHBAUER,
U. 2016. Fracture Rates and Lifetime Estimations of CAD/CAM All-ceramic Restorations. Journal of Dental Research, 95, 67-73.
BELLI, R., WENDLER, M., PETSCHELT, A. & LOHBAUER, U. 2017. Mixed-mode fracture
toughness of texturized LS2 glass-ceramics using the three-point bending with eccentric notch test. Dental Materials, 33, 1473-1477.
BELLI, R., WENDLER, M., PETSCHELT, A., LUBE, T. & LOHBAUER, U. 2018. Fracture
toughness testing of biomedical ceramic-based materials using beams, plates and discs. Journal of the European Ceramic Society, 38, 5533-5544.
FALACHO, R. I., MELO, E. A., MARQUES, J. A., RAMOS, J. C., GUERRA, F. & BLATZ, M.
B. 2023. Clinical in-situ evaluation of the effect of rubber dam isolation on bond strength to enamel. Journal of Esthetic and Restorative Dentistry, 35, 48-55.
FRANKENBERGER, R., HEHN, J., HAJTO, J., KRAMER, N., NAUMANN, M., KOCH, A.
& ROGGENDORF, M. J. 2013. Effect of proximal box elevation with resin composite on marginal quality of ceramic inlays in vitro. Clinical Oral Investigations, 17, 177-83.
FRANKENBERGER, R., MÖRIG, G., BLUNCK, U., HAJTÓ, J., PRÖBSTER, L., AHLERS,
M. O. 2007. Präparationsregeln für Keramikinlays und -teil- kronen unter besonderer Berücksichtigung der CAD/CAM-Technologie. teamwork Journal of Continuing Dental Education, 6, 684-690.
GUAZZATO, M., ALBAKRY, M., RINGER, S. P. & SWAIN, M. V. 2004. Strength, fracture
toughness and microstructure of a selection of all-ceramic materials. Part I. Pressable and alumina glass-infiltrated ceramics. Dental Materials, 20, 441-448.
LAWSON, N. C., JANYAVULA, S., SYKLAWER, S., MCLAREN, E. A. & BURGESS, J. O.
2014. Wear of enamel opposing zirconia and lithium disilicate after adjustment, polishing and glazing. Journal of Dentistry, 42, 1586-91.
LOHBAUER, U. B., RENAN; WENDLER, MICHAEL 2018. Einfluss der Politur auf die Festigkeit zahnfarbener Dentalmaterialien. Quintessenz Zahntechnik, 44, 1546-1559. MARAVIC, T., MAZZITELLI, C., MANCUSO, E., DEL BIANCO, F., JOSIC, U., CADENARO,
M., BRESCHI, L. & MAZZONI, A. 2023. Resin composite cements: Current status and a novel classification proposal. Journal of Esthetic Restortorative Dentistry, n/a. SERBENA,
F. C., MATHIAS, I., FOERSTER, C. E. & ZANOTTO, E. D. 2015. Crystallization toughening of a model glass-ceramic. Acta Materialia, 86, 216-228.